What is diphtheria?
Diphtheria is an infection caused by the bacteria Corynebacterium diphtheriae. Initial symptoms include sore throat, low-grade fever, malaise and swollen lymph nodes on the neck. It most commonly affects the throat, but the toxin released by the bacteria can also cause inflammation of the heart (i.e. myocarditis, 22% of all cases), nerves (i.e. neuritis or localized paralysis, 5% of all cases), kidneys (severe cases only) and skin. Cutaneous (i.e. skin) diphtheria results in chronic, non-healing sores.
The term diphtheria comes from the Greek word for “leather” because of the leathery-looking pseudomembrane (i.e. coating) the bacteria creates on the throat. This coating can get so thick in some children that it blocks the airway and makes it difficult to swallow and breathe. Interestingly, the French physician Pierre Bretonneau (1778-1862) who gave diphtheria its name, was the first physician to record the successful use of tracheostomy, and did so to preserve an airway and save the life of a patient with diphtheria.
How is diphtheria spread?
Diphtheria is spread through contact with respiratory tract mucous/fluid. Contact can be direct through kissing, sharing eating utensils, cups or straws, or indirect through breathing airborne droplets after an infected individual coughs or sneezes. An untreated individual is contagious for two weeks. Treated individuals are contagious until approximately 5 days of appropriate antibiotic use.
Incubation period (i.e. time from exposure to development of symptoms) is relatively short: 2-5 days.
Can diphtheria be treated?
Yes, but treatment typically requires IV anti-toxin to counteract the toxin already produced by the bacteria at the time of diagnosis, as well as antibiotics to kill the bacteria, prevent further toxin production, and decrease contagiousness. Depending on the extent of the pseudomembrane in the throat and the resulting swelling/inflammation, a breathing tube is sometimes inserted to preserve an open airway and prevent the need for a tracheostomy.
How common was diphtheria prior to vaccine availability?
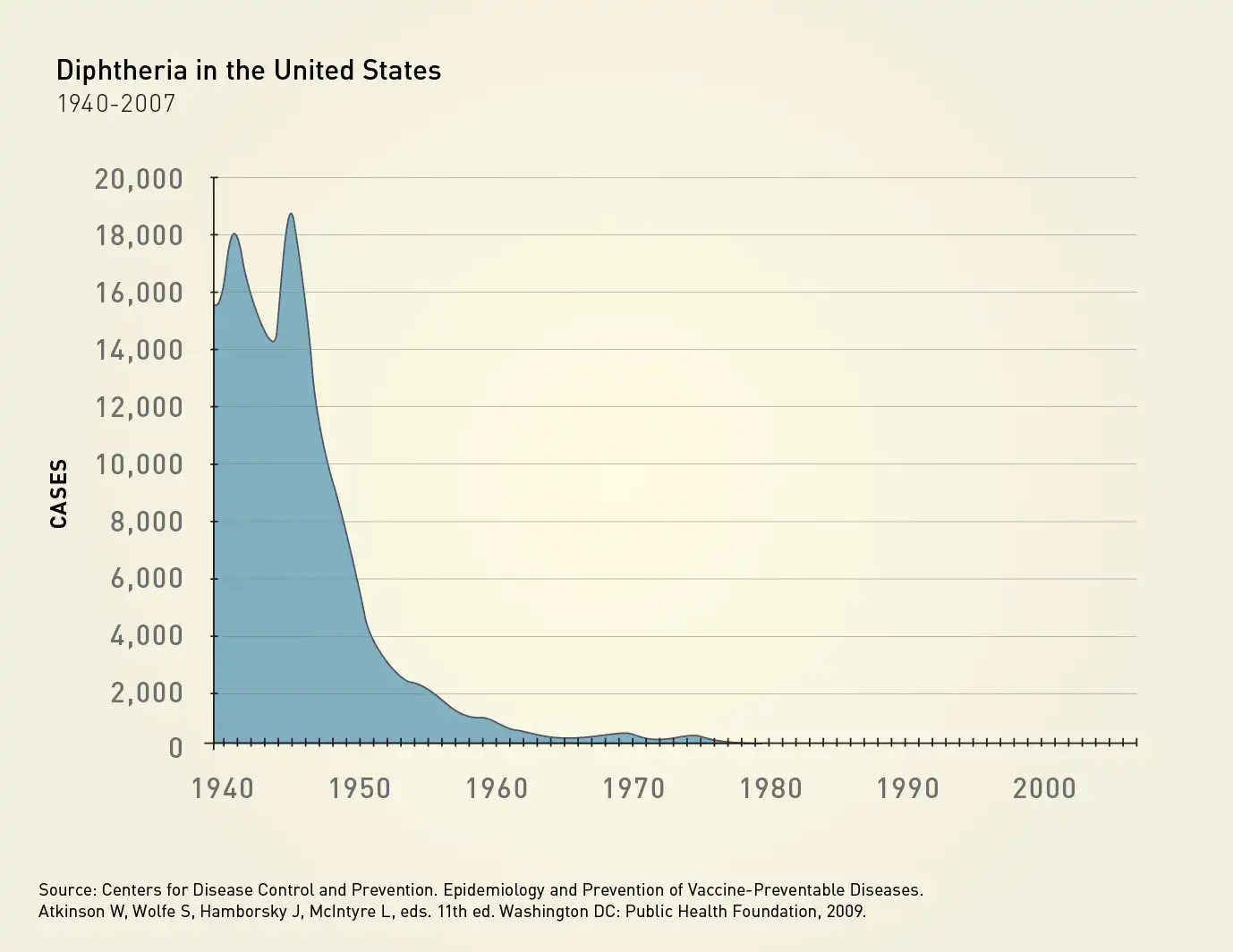
At its peak in the 1920s, diphtheria caused an estimated 150,000-200,000 cases per year, and affected as many as 10% of children. 5-10% of infected children died due to complications of the infection. Introduction of the diphtheria toxoid vaccine in the 1940s led to a significant decline in cases, and has virtually eliminated the disease in the United States, where there is an average of fewer than 1 case per year.
What type of vaccine is the diphtheria vaccine?
Because most of the effects of C.diphtheriae result from the toxin the bacteria produces, the diphtheria vaccine is referred to as a toxoid vaccine. Scientists isolate and inactivate the toxin, resulting in a “toxoid” vaccine that our immune systems can recognize, make antibodies against, and neutralize. Toxoids, unlike the toxin, cannot cause disease, but creates a comparable immune system response. The tetanus vaccine is also a toxoid vaccine.
When do children receive the diphtheria vaccine?
Vaccinating pregnant mothers with a Tdap vaccine passively protects young infants until they are old enough to be actively protected. Antibodies made by the pregnant mother will cross the placenta. Infants receive their first diphtheria vaccine at the 2 month old check-up. Additional doses are administered at 4 months, 6 months, 15 months, and 4-6 years old. Some immune boosting occurs when patients receive their Tdap booster at 11 years old, and every 10 years thereafter. For reduction of side effects and number of total shots, Pediatric Associates of Richmond recommends diphtheria toxoid as part of combination vaccines called Pentacel (for infants and toddlers) and Quadracel (pre-Kindergarten). Isolated diphtheria toxoid vaccine is no longer available in the United States; only as part of one of DTaP, Tdap, or Td.
What’s the difference between DTaP, Tdap, and Td?
DTaP (Diphtheria, Tetanus, acellular Pertussis) The capital letters denote greater immune system stimulation, which is needed at younger ages (less than 6 years old). The significance of “acellular” is reviewed in the pertussis blog post.
Tdap (Tetanus, diphtheria, acellular pertussis) For tweens and older. Full tetanus booster. Has less diphtheria and whooping cough (pertussis) immunity boosting than DTaP because of less need for individuals at that age, but still some need for maintaining herd immunity.
Td (Tetanus, diphtheria) See above, but without pertussis boosting.
What are possible side effects of the diphtheria vaccine?
The diphtheria toxoid vaccine is always combined with at least one other component, so isolating the effects of the diphtheria component from the others is tricky. That said, Pentacel, which Pediatric Associates of Richmond administers at 2, 4, 6 and 15 months old, most commonly causes temporary fussiness, irritability, and crying. These side effects typically last minutes, but in rare cases could last up to 3 hours. With each subsequent dose, the likelihood of these side effects decreases more and more. Inversely, fever can happen in 6% of those receiving their first dose and increase in each of the subsequent 2 doses to a max of 16% of patients receiving their third dose. Injection site tenderness is experienced by about 50% while swelling or redness occur in only 7%.
Quadracel, administered at ages 4-6 years old, causes injection site pain in 75%, redness in 60%, swelling in 40%, muscle aches in 50%, fatigue in 35%, headache in 15% and fever in 6%.
Concluding a 14-month journey through vaccine-preventable illnesses
With diphtheria we now conclude our vaccine blog series “What is it and why is there a vaccine?,” highlighting all the vaccine-preventable infections against which we protect through vaccinations during routine check-ups of infancy, childhood and adolescence. We hope the content has been informative and helpful. Our pediatricians welcome conversations about vaccine benefits and possible side effects. If you have questions at your child’s check-up, please ask!
The short- and long-term data support the effectiveness of vaccines to prevent unnecessary illness. The low risk of possible side effects are dramatically outweighed by the benefit of preventing the infections and the complications they cause.
The pediatricians of Pediatric Associates of Richmond, therefore, strongly recommend these routine childhood immunizations.
We invite you to revisit these blogs prior to check-ups, especially the 1 month, 2 month, 12 month and 11 year old visits (i.e. visits when they may be receiving a particular vaccine for the first time). May the blogs remind you of all the germs and their complications that once made children extremely sick, and which your children will hopefully never have to experience. In order of recommended administration timing, below are each of our blogs:
Tetatus, Diphtheria, Pertussis, Polio, Hib, Pneumococcus, Rotavirus
Measles, Mumps, Rubella, Chickenpox, Hepatitis A
References
2024. “Diphtheria”, Red Book: 2024–2027 Report of the Committee on Infectious Diseases, Committee on Infectious Diseases, American Academy of Pediatrics, David W. Kimberlin, MD, FAAP, Ritu Banerjee, MD, PhD, FAAP, Elizabeth D. Barnett, MD, FAAP, Ruth Lynfield, MD, FAAP, Mark H. Sawyer, MD, FAAP
https://www.uptodate.com/contents/clinical-manifestations-diagnosis-and-treatment-of-diphtheria
https://www.uptodate.com/contents/epidemiology-and-pathophysiology-of-diphtheria
https://historyofvaccines.org/history/diphtheria/overview